Classified as the most aggressive brain cancer by the WHO, glioblastoma is defined by how fast it grows, where it strikes, and how hard it fights back against treatment.
Of all the brain tumors doctors encounter, glioblastoma occupies a category of its own. The World Health Organization classifies it as a grade 4 astrocytoma, the highest and most dangerous tier on a scale that runs from one to four. It originates in astrocytes, the star-shaped supportive cells woven throughout brain tissue, and it does not behave like a single, coherent mass. Glioblastoma contains multiple distinct cell types within the same tumor, a property called heterogeneity that makes it extraordinarily difficult to treat. Target one cell population and others survive, adapt, and continue growing.
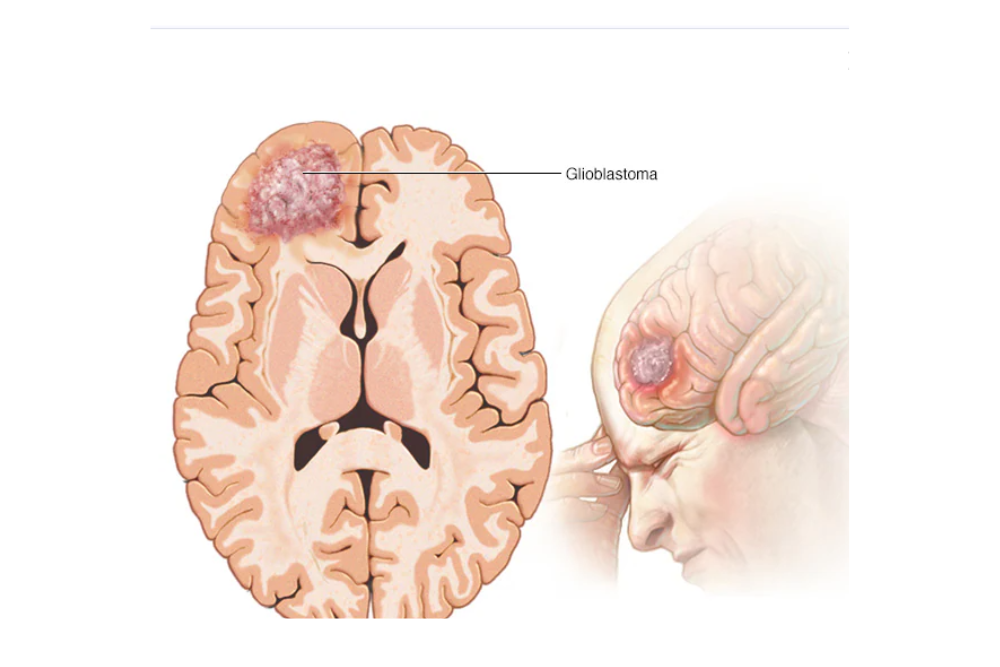
How tumor location shapes glioblastoma symptoms
Where a glioblastoma develops in the brain determines much of what a patient experiences. A tumor in the frontal lobe can alter personality, strip away inhibitions, and cause weakness along one side of the body. One in the parietal lobe may interfere with speech, writing, and spatial awareness. Temporal lobe involvement tends to affect memory and language comprehension. Tumors near the occipital lobe often cause visual disturbances or partial vision loss, while those affecting the cerebellum disrupt balance and fine motor control. Tumors near the brain stem carry the most serious consequences, including effects on breathing, heart rate, and blood pressure.
The most common symptoms across tumor locations include persistent headaches that tend to worsen in the morning, seizures, cognitive changes, nausea, one-sided weakness or numbness, and shifts in personality or behavior that can be mistaken for psychiatric conditions before a diagnosis is made.
Who develops glioblastoma and why
The causes of glioblastoma are not fully understood. Certain inherited genetic syndromes, including Li-Fraumeni syndrome and Turcot syndrome, elevate a person’s risk. Prior radiation therapy to the brain is also associated with increased risk. The disease is more common in adults over 50 and occurs somewhat more frequently in men than in women, though it can develop at any age.
Diagnosing glioblastoma
Diagnosis begins with a neurological examination to assess cognitive and physical function, followed by magnetic resonance imaging, which remains the standard tool for detecting and mapping brain tumors. MRI provides enough detail to identify tumor size and location, but a definitive diagnosis still requires a biopsy. A tissue sample is examined under a microscope to confirm the presence of cancerous cells and establish the grade.
Treatment options for glioblastoma patients
Treatment typically involves surgery first. Surgeons attempt to remove as much of the tumor as possible, a process called resection, though complete removal is rarely achievable given how deeply glioblastoma infiltrates surrounding brain tissue. Radiation therapy follows to address remaining cancer cells, and the chemotherapy drug Temozolomide is generally administered alongside and after radiation as standard of care.
Bevacizumab, sold under the brand name Avastin, is a targeted therapy that works by inhibiting the growth of blood vessels feeding the tumor. Tumor Treating Fields therapy, a newer approach, delivers low-intensity electrical fields through pads placed on the scalp. Used in combination with chemotherapy after radiation, it has shown the ability to disrupt cancer cell division without significant systemic side effects.
Clinical trials remain an important avenue for patients whose disease has progressed beyond standard treatment. Immunotherapy and gene therapy are among the experimental approaches currently under investigation. The registry at ClinicalTrials.gov maintains an updated list of active studies.
Glioblastoma is a diagnosis that demands immediate, coordinated care from a specialized neuro-oncology team. No two cases are identical, and treatment plans are shaped by the specific biology of the tumor as much as by its location and grade.




