Most people have had a mouth ulcer. The familiar small sore that appears after biting the inside of a cheek, irritation from a sharp tooth, or friction from an ill-fitting denture. It stings, it heals within a week, and it gets forgotten. That pattern covers the majority of cases. What concerns clinicians is the minority that does not follow it.
Any ulcer that persists beyond three weeks warrants a biopsy or further investigation. The reasons range from chronic infections to malignancy, and waiting out a sore that shows no sign of closing is not a reasonable approach.
What causes mouth ulcers
Trauma is the most common cause, and its ulcers resolve quickly once the source of irritation is removed. Rinsing with a chlorhexidine mouthwash supports oral hygiene during healing, and benzydamine hydrochloride spray or mouthwash can manage discomfort in the meantime.
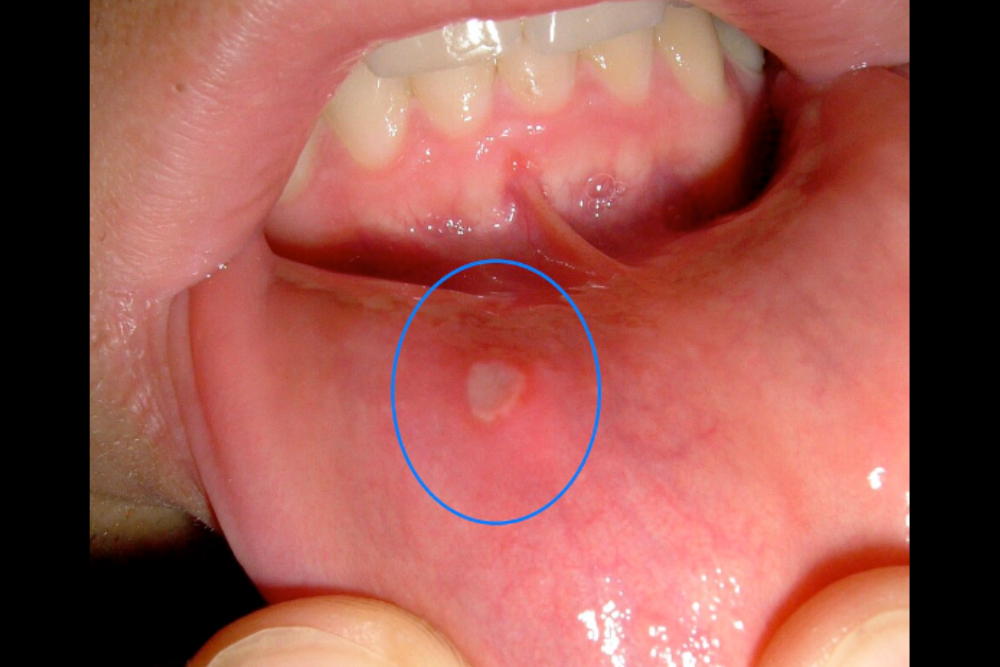
Recurrent aphthous stomatitis, more commonly known as canker sores, is a separate category entirely. It affects at least 20% of the population and typically begins in childhood or adolescence. The ulcers are round or oval with defined edges, a red border, and a yellow or grey surface. Three main forms exist. Minor aphthae, which account for about 80% of all cases, are smaller than 5 mm and heal within 7 to 14 days. Major aphthae are larger, heal slowly over weeks or months, and can leave scarring. Herpetiform ulcers appear as clusters of small pinpoint sores and generally clear within a month.
Most people with recurrent aphthous stomatitis are otherwise healthy, but a meaningful subset has identifiable contributing factors. These include stress, hormonal changes, nutritional deficiencies involving iron, folate, or vitamin B-12, and conditions like celiac disease, Crohn’s disease, and HIV infection. Behcet’s syndrome is associated with frequent, severe episodes that take a long time to heal and may also involve ulcers in other parts of the body.
Management typically starts with identifying and addressing any underlying factors. Chlorhexidine mouthwash can help. Topical corticosteroids applied several times daily are often effective at controlling symptoms. More severe or frequent cases may require systemic treatment under specialist supervision.
When ulcers signal something systemic
Ulcers that appear without obvious trauma or a pattern consistent with aphthae may reflect an underlying systemic condition. Skin disorders including lichen planus, pemphigus, and pemphigoid can all produce oral lesions. Blood disorders including anemia, leukemia, and neutropenia are also associated with mouth ulcers, as are gastrointestinal conditions like ulcerative colitis and Crohn’s disease. Certain medications, particularly cytotoxic agents and the cardiac drug nicorandil, can also be responsible.
Burning pain and other non-ulcerative conditions
Not all oral soreness involves visible ulcers. Erythema migrans, sometimes called geographic tongue, produces map-like patches of redness on the tongue that shift in location over hours or days. It affects roughly 10% of children and adults, causes soreness in some people and no symptoms in others, and has no reliably effective treatment. It carries no serious implications in most cases.
Burning mouth syndrome is more common in people past middle age and produces a persistent bilateral burning sensation in the tongue. Its cause is not fully understood, but the fact that it responds to topical anesthesia suggests a neurological basis. Unlike ulcer pain, which worsens with eating, burning mouth discomfort is sometimes relieved by food and drink. Organic causes including candidiasis, nutritional deficiencies, dry mouth, and diabetes should be ruled out before attributing the condition to psychological factors, though anxiety and depression are frequently involved. Antidepressants are sometimes indicated.
Orofacial pain beyond the mouth
Pain in and around the face and jaw extends beyond ulcers and mucosal soreness. Temporomandibular joint pain-dysfunction syndrome primarily affects younger women and produces clicking, limited jaw movement, and muscle tenderness around the joint. Bruxism, the habit of clenching or grinding the teeth, is a common contributing factor. Most patients recover with conservative measures including rest, jaw exercises, soft diet, and over-the-counter pain relief. A small number require more targeted intervention.
Atypical facial pain and atypical odontalgia are less well understood. They present with chronic, poorly localized discomfort that does not correspond to identifiable dental pathology. Antidepressants have shown benefit in some patients, though many are resistant to both medication and psychological support.




